
Minority Reproductive Care At Risk
Ending funding of Planned Parenthood will mostly hurt minority patients in city.

Women of color in Milwaukee will be disproportionately harmed by a provision in the American Health Care Act ending Medicaid reimbursements for abortion providers, such as Planned Parenthood. This could result in severely limited services such as gynecological exams, STD testing and treatment, and contraception. Photo by Naomi Waxman.
Until she was 20, Tiferet Berenbaum, 34, had never seen a gynecologist. She had never had a Pap smear, or even heard of one.
In 2003 Berenbaum, a college sophomore, made her way to a nearby Planned Parenthood health center to learn about her contraceptive options.
“When I went to get on the pill they made it clear that part of the deal is I had to get examined before and yearly in order to keep up the prescription,” she said.
The Pap smear results came back showing the presence of pre-cancer cells that could grow into cervical cancer. Berenbaum underwent a procedure to remove the cells and hasn’t had a ‘bad Pap’ since.
“Just left to their own devices, those kinds of things can escalate into a more serious problem,” she said. “Planned Parenthood really saved my life. I would have never gone on my own to get any kind of feminine exam if I hadn’t stumbled into Planned Parenthood.”
Berenbaum, who is African-American, knows she was lucky her condition was caught early so she was able to receive treatment and start seeing a doctor regularly.
Unfortunately, many women of color in Milwaukee are not so lucky.
Low-income Milwaukeeans, who already face significant barriers to accessing reproductive health care services, would be disproportionately affected by cuts to health care funding passed by the U.S. House of Representatives in early May, which are awaiting a vote in the Senate. According to a 2015-16 Milwaukee Health Department (MHD) report, 39 percent of African-Americans, 31.8 percent of Hispanics and 14.8 percent of non-Hispanic whites in the city live in poverty.
The American Health Care Act (AHCA) includes a provision that will bar Planned Parenthood or any other reproductive healthcare provider that performs abortions from Medicaid reimbursement. The cuts would force clinic closures across the state and leave the six in 10 Wisconsin Planned Parenthood patients who are covered by Medicaid in peril. Forty-eight percent of Planned Parenthood patients in Milwaukee County are African-American (see graphic, below).
Though it is not explicitly under attack by the AHCA, health advocates also fear for the Title X Family Planning Program, which makes reproductive health care available to low-income women at low or no cost. President Donald Trump signed a bill in mid-April that altered how some states distribute Title X funds, but Wisconsin is not among the affected states for the time being.
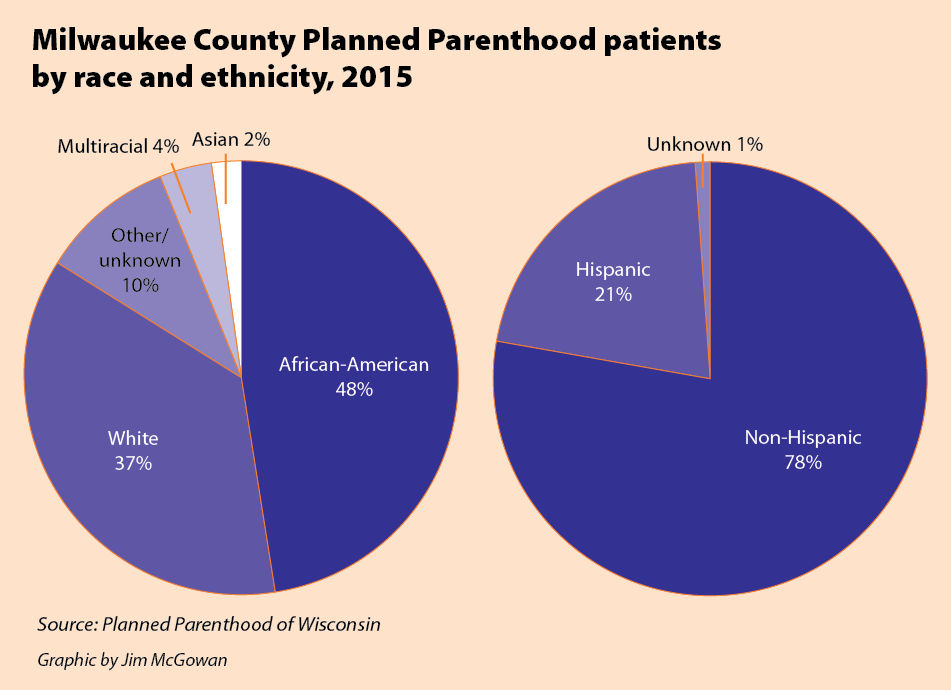
Milwaukee County Planned Parenthood patients by race and ethnicity, 2015
In Milwaukee County, 76,210 women between 13 and 44 require access to reproductive health care services including contraceptive care and sexually transmitted infection testing and treatment, according to the Guttmacher Institute. Currently, 34,600 women receive these services at publicly funded health centers, leaving the remainder without access to services, highlighting the already-significant need in the city, according to Planned Parenthood, which has six health centers in the county.
Reproductive health care is a catchall term for a variety of services including gynecological exams, STD testing and treatment, contraception, pregnancy testing, prenatal care, birth care and abortion. It has long been a political battleground in the United States in regard to public funding for services — especially abortion.
While reproductive health is essential for emotional and physical well-being, low-income residents face barriers to obtaining clinical health care services. Chief among them is cost: 16 percent of households in the city stated one or more members were not covered by health insurance anytime in the previous year, according to the 2015-16 MHD report. Other obstacles include access to transportation, appointment delays and cultural gaps between patients and providers.
These barriers result in less likelihood that women of color will receive preventive screenings, a survey by Planned Parenthood found. Consequently African-American and Latina women are generally diagnosed with cancer at later stages and experience poorer health outcomes than non-Latina white women.
Nationwide, African-American women are twice as likely to die from cervical cancer than non-Latino white women and 40 percent more likely to die from breast cancer, according to research by the Kaiser Family Foundation and the National Women’s Law Center.
Cultural barriers to care, in concert with logistical obstacles, contribute to these poor health outcomes. Though a doctor, nurse, clinician or educator may be well intentioned, he or she may make assumptions regarding behavior and lifestyle that can alienate women of color and ultimately discourage them from seeking care.
Danielle Taylor, 33, was 19 years old and five months pregnant when she began experiencing abdominal pain. Concerned about the fetus’ health, she made an appointment to see an OBGYN at St. Joseph and described painful cramping sensations. Before examining her, however, the doctor began to theorize about what might be the cause.
“She goes, ‘You know, it’s most likely you’ve got a disease…All of you guys usually have a disease.’”
Stunned, Taylor told the doctor that she had regular checkups and was sure that she did not have a sexually transmitted infection. Still, she said, the doctor insisted. Taylor, now angry and upset, began to argue with the doctor and the conflict quickly escalated into a shouting match.
“It got really ugly,” said Taylor, a Harambee resident.
The doctor was eventually removed from the room, she said, and hospital staff offered to have another doctor examine her, but did not apologize. She did not hear from the hospital again.
Taylor said that the experience was so traumatic that she began avoiding interactions with the health care system. She now wishes she had filed a complaint with the hospital, but at such a young age she didn’t know where to begin.
“After that I kind of dropped my OB appointments … I didn’t want to be bothered with even going to the doctor,” she said. “I don’t know if [I was treated this way] because I’m African-American or because I’m on state insurance or a combination of both.”
Taylor’s negative experiences with providers have continued throughout her life.
An African-American mother of eight, Taylor recently told her physician that she had problems using an IUD (intrauterine device) in the past and wanted a different form of contraception.
“The doctor said, ‘Let me tell you, you’re going be pregnant with number nine next time you come in here,’” said Taylor.
Dominique Alvarado, 21, had a similar experience when she decided that she did not like the side effects of hormonal birth control on her body. Much to her surprise, when she visited her gynecologist to discuss her concerns, she was greeted with opposition and a distinct feeling that she was being judged.“We were almost arguing about the fact that I wanted to go off my birth control,” Alvarado said. “From then on I have not gone back. I went to Planned Parenthood … because I didn’t want to schedule an appointment with that OBGYN.”
These cultural gaps occur both in and outside the exam room, affecting a wide variety of services that are designed to benefit pregnant women and parents.
When Alvarado, who lives on the South Side, became pregnant with her son Zaylyn, her doctor encouraged her to take birthing and parenting classes. She attended a few sessions, but felt out of place and isolated.
“From what I saw at the hospital, it was primarily middle-class white couples who were married … I didn’t have a partner. I didn’t want to socialize with these people because we have nothing in common.”
In retrospect, she said that she would have attended more classes if they were designed for single parents or women of color.
Raina Johnson also recalled attending a parenting class made up predominantly of white women where she was assured that friendly neighbors and community members would donate clothes, blankets and food after she gave birth.
“I remember going to these classes and thinking, ‘What are they talking about? Who is this magical village of people who are going to give me things?’” said Johnson.
Johnson, 31, recalls the confusing and overwhelming early days of motherhood in stark contrast to the rosy picture painted in the parenting classes she attended.
“None of [those things] happened for me. I bought everything. I didn’t have a baby shower. No one brought me a casserole. I didn’t have a mother-in-law to come stay with me for two weeks after the baby is born.”
Maria Barker, multicultural programs manager at Planned Parenthood of Wisconsin, said that patients of color or who are on Medicaid frequently report negative experiences with health care providers.
“I hear from people all the time how [the doctor] … is OK with providing them service and [the patient was] treated OK but the frontline staff and nurses treated them like garbage for having state insurance and being poor,” Barker said.
These patients, she said, are made to feel as if the provider is doing them a favor by caring for them.
“Some providers [make] assumptions about people on Medicaid and without insurance,” said Planned Parenthood clinician Jody Krahn, echoing Barker’s assessment. “Over time, if people are treated badly for whatever reason in the healthcare system, they form a hard shell and it’s difficult to get through to them.”
Threats to funding
As daunting as these obstacles might be, they are going to get worse if the federal government cuts off Medicaid funding for Planned Parenthood, an element of the AHCA.
This could be devastating for low-income Milwaukee women, said Nicole Safar, policy director at Planned Parenthood Wisconsin.
“If we didn’t have that source of payment for the services provided, it’s very likely that we would not be able to maintain a statewide network of 19 [family planning] clinics,” which serve 60,000 patients throughout Wisconsin, she said. “We serve about 30,000 patients in Milwaukee and … all of those could lose their access to health care.” Planned Parenthood has five health centers in Milwaukee, only one of which provides abortions.
Only three clinics provide abortions in Wisconsin. Two are located in Milwaukee, including the Planned Parenthood clinic, while the third is in Madison. Telemedicine abortions, or over-the-phone abortion pill prescriptions issued by a licensed physician, are banned in the state.

(From left) Rabbi Noah Chertkoff, the Rev. Andrew Warner, the Rev. David Dragseth and Rabbi Tiferet Berenbaum. Photo by Naomi Waxman.
In a bizarre twist, clinics that offer abortions are supported entirely through private funding and donations, so health care centers that offer other family planning services but not abortion will bear the brunt of the cuts.
The 1976 Hyde Amendment prohibits the use of federal Medicaid funding for abortion services, but states enjoy some leeway when it comes to how to use state Medicaid funds. Unlike neighboring state Minnesota, Wisconsin also prohibits use of state funds for abortion care.
“Under [federal and state law], Medicaid cannot pay for abortion services. It is the one health care service that is carved out of the Medicaid program,” said Safar.
A woman who is otherwise eligible for state medical assistance is banned from receiving public funding for abortion unless the procedure is necessary to save her life, is necessary due to an existing condition that may endanger her life, or is a victim of rape or incest who can provide a police report documenting the assault.
NARAL Pro-Choice America assigned the state a D+, or “severely restricted,” in its annual state-by-state review of abortion services, and noted that legislation disproportionately affects low-income women.
Wisconsin women do have access to some state assistance for reproductive health care. The Family Planning Only Services Program benefits low-income women but fails to cover some services, including mammograms, hysterectomies and inpatient treatment.
Under Wisconsin law, health insurance plans that cover prescription medication are required to provide the same coverage for FDA-approved contraception. Employers that provide insurance for prescriptions are also subject to this requirement.
If the AHCA cuts funding for Planned Parenthood, many wonder where Wisconsinites will go who now rely on the organization for comprehensive reproductive health care.
Legislators opposed to Planned Parenthood, including House Speaker Paul Ryan, have stated that Federally Qualified Health Centers (FQHCs) could serve clients who would lose access to care should clinics close as a consequence of cuts to Medicaid.The American Congress of Obstetricians and Gynecologists disagrees, writing in the Annals of Internal Medicine that “forcing the closure of Planned Parenthood health centers would put immense pressure on private and unaffiliated health care providers … to assume care for patients previously seen at those clinics while their own practices already are at full capacity.”
Safar said that FQHCs in Wisconsin have clearly stated that they cannot accommodate the patients PPWI serves across the state. “They don’t have capacity to absorb significant [numbers] of new patients.”
Safar also expressed concern for the future of the federal Title X Family Planning Program, enacted in 1970, which makes some clinical services available at no cost to patients at or below the federal poverty level, while those with incomes between 200 and 250 percent of the federal poverty level are charged on a sliding scale.
Nationally, women of color constitute more than half of the 4 million family planning clients served by Title X, according to the Center for American Progress.
“[The Title X program] in general is at risk under this [presidential] administration and Republican leadership in Congress,” Safar said. “The existence of the overall program is something that we’re concerned about losing when we have an administration that doesn’t support access to family planning.”
Stigma
In 2010, Raina Johnson was still adjusting to parenthood. Her son Elijah, then 6 months old, resulted from an unplanned pregnancy and Johnson was raising him without a partner. At 24, the Milwaukee native had just celebrated her graduation from Cardinal Stritch University and suddenly found she was staring down the long barrel of student debt.
“I was in survival mode, the mode a lot of black women operate in,” Johnson said.
She subsequently discovered that she was pregnant again. Johnson knew that given her finances and Elijah’s young age, caring for another infant was not an option for her.
“The recession was terrible and I have a degree [in English] that doesn’t make a lot of money so I didn’t have any real prospects,” said Johnson. “The decision to terminate the pregnancy… was the best decision for me.” She published an essay about her experience titled, “I had an abortion because I love my son.”
Johnson said she was grateful that she was able to find money for a termination and obtain non-judgmental care at Planned Parenthood. “Planned Parenthood was great and I was able to scrounge up the money and make it work,” she said.
Johnson had no personal qualms about seeking an abortion, but she still felt the stigma associated with the procedure.
“I felt very ashamed because I had achieved this pinnacle of a college degree so I felt like I couldn’t go to [my family] with this disappointment. … I didn’t want to bring a dark cloud over [my academic accomplishments],” she said.
Wisconsin requires women seeking abortions to jump through a series of strategically placed hoops, including attending in-person counseling designed to discourage patients from terminating a pregnancy. State law dictates that clients must then wait 24 hours before the abortion, necessitating two trips to the facility. Childcare costs, transportation and obtaining time off work for procedures and recovery are among the obstacles facing low-income patients, which are significantly exacerbated by the state-mandated waiting period.
Dominique Alvarado said that in her experience, communities of color do not always regard abortion as a viable option, regardless of legality or accessibility.
“In the culture of Latino and even African-American communities, it’s like, ‘This is what you did so this is your life now.’ … For many women of color, there are no options — you were sexually active so now you’re going to parent.”
African-American and Hispanic women have abortions at significantly higher rates than white women nationwide and also face among the highest rates of unintended pregnancy. Abortion rates relate directly to the rate of unintended pregnancy, and women who are minorities or live in poverty encounter particularly high barriers when trying to access contraception, researchers from the Guttmacher Institute found.
In her work as a Planned Parenthood peer educator as an adolescent, Alvarado interacted with many youth of color seeking information about how to protect themselves from unplanned pregnancies and sexually transmitted infections.
“A lot of them grew up in very controlling environments where they didn’t know they could come somewhere like Planned Parenthood without their parents’ consent and access [the services] they needed,” she said.
“You have this environment where you’re told, ‘You better not bring any kids into my house,’ yet you can’t talk to your parents about accessing things like birth control or condoms.”
Sex education programs, if present in a school at all, vary wildly across the country: only 13 states require that the information presented to students be medically accurate. Wisconsin is not among them. Although it can be difficult for teenagers to get information about reproductive health in school, PPWI offers home health parties to discuss this issue. Maria Barker developed the program in 2004.
“My frustration allowed me to think outside the box. Who has power to give me access to young people? Parents!” said Barker.
Inspired by Tupperware and Avon parties, she began holding informal meetings with local parents at their homes to discuss strategies for communicating with young people about reproductive health.
Barker quickly found that parents were much more interested in bringing her in to speak directly with their teenagers than in initiating these conversations themselves. Thirteen years later, Planned Parenthood holds approximately 500 home health parties per year with the assistance of a cadre of community health workers.
“You don’t know what you don’t know,” Barker added. “Once someone gives you a safe place in which to have real conversation about a real thing like … reproductive health and how to speak up for yourself, who wouldn’t want to do it?”
Concern for the future
Four months ago, 14 years after pre-cancerous cells were identified in her first Pap smear, Tiferet Berenbaum gave birth to a healthy baby girl at Aurora Sinai Medical Center. That same month, House Republicans were preparing the initial version of the AHCA, which failed to pass.
Berenbaum believes it is unlikely she would have received such a high level of care if the current bill were in effect when she delivered.
“I probably wouldn’t have had the level of comprehensive health care I needed and would have had to cover the bulk of delivery, so I would be in debt right now,” she said. “I don’t know what I would have done.”
Berenbaum had a cesarean section, a procedure not explicitly addressed by the AHCA but one that insurers have identified in the past as grounds for charging higher premiums. This, too, makes her worry about the costs associated with future pregnancies she may have.
“I feel like a target,” she said. “I feel like my health care needs and requirements are being milked for profit. I’m thinking about my daughter all the time and I’m just praying that she doesn’t have to pay a higher price just because she’s a woman.”
This story was originally published by Milwaukee Neighborhood News Service, where you can find other stories reporting on fifteen city neighborhoods in Milwaukee.


















What a comprehensive and informative article. Thanks Naomi!
I think the irony is lost on too many people…..minority women clamoring for access to an organization that has the eradication of minorities from America as its founding principle.
Oh good, I was wondering if anyone was still pretending that Planned Parenthood provided prenatal care.
But hey, some people had a bad experience with their OBGYN, so let’s fund an organization who’s main service for pregnant women is abortion.
The fact that Planned Parenthood still gets a pass on their eugenic roots, their continuation of disproportionately targeting minority women for abortion (abort, don’t support), their proven false assertions of the ob-gyn services they provide, and their profiting from the selling of human body parts astounds me. I suggest a viewing of MAAFA 21 is in order. We can offer minority women so much more than the “choice” to kill their unborn children!
Anne, take your easily debunked lies elsewhere.
http://www.snopes.com/margaret-sanger-weeds/
“A quote falsely attributed to birth control advocate Margaret Sanger likens Slavs and Jews to human “weeds” in need of eradication.”
Tim, even better than Snopes are the primary sources I own. I invite you to do some credible research.
Abortion is legal (as it should be). Sorry if that hurts your ears AG. And the fact of the matter is closing PP clinics hurts poor women and women of color. Not that you care, but it does. Of course as a man you really should be in charge of legislating reproductive health matters.
Anne Haines, where is your proof? I just see baseless accusations, are you even going to copy & paste your chain letter?
As a woman and a feminist I would rather men not be taken out of the equation of what happens with their children. If men are to be held accountable we cannot have it both ways. And, for the record, abortion is not “reproductive health”.
Never said anything about men having no rights or responsibilities. Your proof Anne? Still waiting….
The assumptions (and links) don’t work. If the universe of women needing reproductive health care services in Milwaukee is 74,960 (per the Guttmacher link) and 34,600 receive those services from publicly funded clinics, it doesn’t mean that the difference receive no care. Some of those receive no care but I’d surmise that the majority use private insurance. The link related to the 34,600 is broken.
Anne, thank you, I completely agree. It is up to all women and men who have an ounce of compassion for life to stand up for the rights of innocent unborn children who are being murdered. It is sad that third wave feminists would silence true feminists, including men, just because of their blind support for legalized killing of unborn children. Unfortunately, people like Vincent have actually convinced themselves that people who support all life somehow don’t care about women and children.
I’d still love to hear how abortions are “reproductive health” or how articles like this can continue to pretend that PP provides prenatal care. Still waiting…